
Beyond single causes for a deeper understanding of suicidal ideation
Why reducing suicidal thoughts requires comprehensive and measurement-based approaches to care.

Suicide is a leading cause of death among young people, but suicidal thoughts rarely arise from a single cause. They are shaped by many factors - mood, social connection, trauma, anxiety, and sleep among many others - and these influences interact and shift over time, making suicidal ideation a dynamic and unpredictable experience.
Recent research from our team is helping us to understand how various clinical and psychosocial factors interact and contribute to suicidal ideation, and how tracking changes in suicidal ideation over time may give us the chance to intervene earlier and prevent a crisis.
In this article, we’ll look at what these findings reveal about suicide risk factors, how digital monitoring can strengthen care, and why a more proactive approach to mental health could be transformative.

A complex network of risk factors
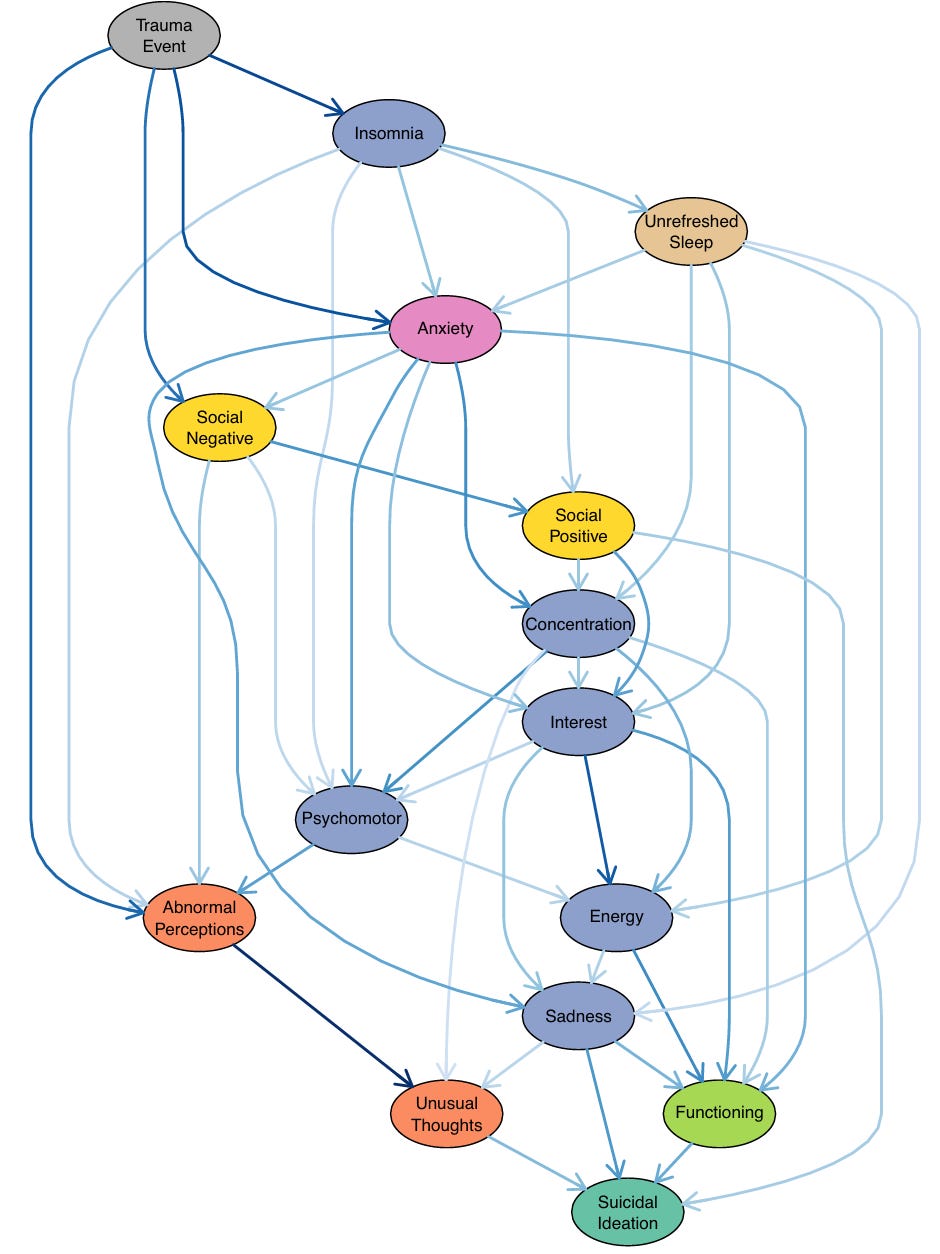
In the first study we used probabilistic graphical models to map how different clinical and psychosocial factors relate. In these models, each factor is a node, and links (or “edges”) between nodes show how factors depend on one another.
We analysed data from 1,020 help-seeking young people (aged 12–25) who were using a measurement-based care platform (Innowell). This platform gathers a wide range of information about mood symptoms, psychosis-like symptoms (e.g. hearing voices or unusual thoughts), social support and connection, functional impairment in daily life, history of trauma, sleep quality, and more. We used this data to explore which factors lead to suicidal thoughts.
Instead of isolating single risk factors, we mapped the full constellation of a young person’s mental health, showing how the pieces interconnect. This allowed us to distinguish between proximal factors (immediate drivers of suicidal thoughts) and distal factors (indirect influences) - see figure below.
The proximal factors were strikingly intuitive yet important to confirm: depressed mood, functional impairment, poor social connection, and psychosis-like experiences. In other words, when a young person is currently feeling intensely sad or depressed, struggling to function in daily life, feeling isolated or unsupported socially, or experiencing psychosis-like symptoms (such as hearing voices or feeling a loss of control over their thoughts), these conditions are most closely tied to having suicidal thoughts. These proximal factors appeared as direct nodes leading into the suicidal ideation node in the network.
Distal factors, by contrast, exert their influence through other problems. Trauma, anxiety, and sleep and circadian factors (like insomnia and feeling unrefreshed by sleep) were especially important, not because they connected directly to suicidal ideation, but because they set off potential cascades which feed into mood problems, isolation, or unusual experiences that could heighten risk.
As you read this article (and look at the figure below), it’s important to note that these models are probabilistic, not deterministic. They highlight patterns and pathways that increase or decrease the likelihood of suicidal thoughts (in a clinical sample), but they do not mean that a person will definitely develop suicidal ideation simply because they have certain factors. Every person’s experience is unique, and risk is shaped by a dynamic interplay of many influences rather than a fixed outcome.
Improving indicated prevention and early intervention
This work has real implications for how we approach mental health care. Proximal factors carry the most immediate information about risk. This means that in a clinical setting, paying close attention to a young person’s current depressive mood, their level of daily functioning, their sense of social connectedness, and any psychosis-like symptoms can give the clearest indication of potential risk.
On the other hand, distal factors provide context and targets for longer-term prevention. These factors might not tell us that the person will develop suicidal thoughts however they indicate vulnerabilities and the paths through which trouble could emerge. For example, the analysis suggests that trauma exerts its influence through a cascade of effects on other problems. This means that for someone with trauma, early intervention can focus on those intermediary problems, such as improving sleep, treating anxiety, and fostering safe social connections.
In practical terms, these insights align with the push for comprehensive youth mental health care. Effective care should consider the whole network of factors affecting a young person. The fact that so many elements - mood, social support, functioning, trauma, anxiety, sleep, psychotic symptoms – are interrelated in contributing to suicidal ideation is evidence that a one-size-fits-all approach is likely to fall short. Integrated care models that cover a broad range of clinical and psychosocial needs are well-suited to address this complexity.
It’s important to note that although suicidal ideation is an important signal of risk, it does not automatically lead to suicidal behaviour. Large-scale studies consistently show that while many young people report experiencing suicidal thoughts, only a smaller proportion will ever attempt suicide. The step from thinking to doing involves additional factors, such as access to means, acquired capability, impulsivity, and decision-making under acute distress, that we still do not fully understand. This transition remains one of the biggest challenges in suicide research.
Despite this uncertainty, focusing on reducing suicidal ideation is still a critical priority for clinical care. Suicidal thoughts are painful and impairing in their own right, disrupting daily life, relationships, and hope for the future. Moreover, lowering the intensity or frequency of ideation is likely to reduce the probability of progression to an attempt, even if it cannot eliminate the risk entirely. For clinicians, this means that addressing suicidal thoughts directly through evidence-based interventions, and bolstering protective factors like social support remains one of the most meaningful ways for indicated prevention and early intervention.
However, implementing truly comprehensive care is challenging. It requires not only thorough initial assessment, but also ongoing monitoring of the person’s status across these domains. This is where technology and measurement-based care come into play, offering new ways to understand a person’s mental health over time.
Why measurement-based care matters
Identifying risk factors is only part of the challenge. The other is timing. Suicidal ideation doesn’t follow a fixed course; it changes, sometimes gradually, sometimes suddenly.
This is why in today’s digital world, technologies that enable measurement-based care are transforming mental health care by enabling continuous tracking of mental health. This is a practice of routinely collecting data on a person’s symptoms, suicidal thoughts, and functioning to inform clinical decisions. Instead of relying solely on sporadic clinic visits, measurement-based care uses structured self-reported outcome measures (through smartphone apps, web portals, text check-ins, etc.) and even passive data from wearables or sensors to create an ongoing record of a person’s mental health.
By shifting from one-off assessments to continuous, digitally enabled monitoring, clinicians gain a more dynamic picture of how something like suicidal thoughts fluctuates, helping to identify when background vulnerabilities are beginning to cascade into immediate warning signs.
But monitoring alone can only take us so far. We need to learn from this information and use it to inform decisions. So, in a second study, continuous-time modelling was applied to learn the unique trajectories of suicidal ideation for 585 individuals using the same measurement-based care platform (Innowell). The result was a dynamic and personalised forecast of where an individual’s mental health might be heading, rather than a one-size-fits-all risk score.

We showed that although there was huge uncertainty early on (when there were few assessment points/red dots), these trajectories could be learned over time. These individual-level trajectory models could tell us about the expected level of future suicidal ideation and its likely variability for a given person.
This has practical implications: if a model predicts that a person’s suicidal ideation is likely to remain low and stable, the clinician might space out appointments and follow-up; but if it predicts high or wildly fluctuating ideation, that person may need more frequent follow-up and contact with services. For this, we derived a metric called “recommended follow-up time (FUT)” for each person – essentially, an estimate of how quickly the person’s data becomes outdated for predicting their state (a shorter FUT means that data loses predictive value quickly, so you need to check in often).
In this way, dynamic tracking enables truly proactive care: instead of reacting after a suicide attempt or emergency, the care team can anticipate and address sharp changes in a person’s risk in real time.
Towards proactive and effective care
Both studies point in the same direction: mental health care must become more comprehensive and dynamic. Comprehensive, because risk comes from both immediate struggles and deeper vulnerabilities (social, biological, behavioural, psychological). Dynamic, because outcomes like suicidal ideation fluctuate, sometimes rapidly, and so care must track these outcomes and adapt accordingly.
Proactive mental health care means not waiting until a young person is in crisis. It means monitoring the shifting landscape of their mental health and wellbeing, recognising when background vulnerabilities begin to cascade into immediate concerns, and stepping in early with the right support. It is clear that for this type of proactive mental health care, we need strong investment in the use of digital technologies that facilitate this level of personalised and measurement-based care.
For young people struggling with suicidal thoughts, this shift could be life-saving. And for the rest of us, it offers hope that even in the complexity and uncertainty of mental health, we are learning how to intervene with greater clarity, precision, and care.